More than one in five Canadians, an estimated 6.5 million people, do not have a family physician or nurse practitioner they see regularly, according to a national survey. I am lucky enough to be able to have a primary care physician (I did lose my previous family doctor during the pandemic), but I know several people who have been on waiting lists for several years.
I recently listened to an inspiring podcast episode from Dr. Tara Kiran detailing the Costa Rican primary care healthcare system and was amazed by their approach to healthcare, which, in my opinion, is truly patient-centred. I highly suggest you listen to the episode, but some of the highlights are:
- The centralized Costa Rican healthcare organization has divided the country into over 100 geographical regions, where each region is connected to a primary care team
- They have a team-based model of primary care. Each multidisciplinary EBAIS (Equipos Básicos de Atención Integral de Salud, which roughly translates to Basic Teams of Comprehensive Health Care) teams consist of a doctor, a medical assistant, a community health worker and a medical data clerk
- Part of the backbone of the EBAIS team are ATAP (Asistentes Técnicos en Atención Primaria), who are community health workers who conduct home visits to the clients assigned in their region
This model is revolutionary because it flips the idea on its head that you should only visit your primary care provider when you are sick, and applies a preventative care lens to healthcare delivery. Not only do these community health workers check for basic clinical measures such as blood pressure, but they also check for and document social determinants of health factors within their electronic medical record, such as: is there stagnant water around the home (could be a risk of malaria)? Does the home have a refrigerator (important for those who need insulin)? This focus and understanding of the patient characteristics of the area you are serving is key, in my opinion, for the collection of accurate and actionable information.
Working in the health informatics field, there can be a rush to collect data without a clear understanding of what the outcome of this data collection will be and how it will make an impact on the communities we are supposed to be serving. Listening to the podcast episode, it is clear that there is a culture and a mutual understanding among healthcare workers that every Costa Rican deserves equitable access to care. To me, it is not just lip service; it is clear in how they have set up their system, both through a holistic approach by enlisting a multi-disciplinary health team (including a medical data clerk) and by documenting their interactions with patients within their electronic medical record.
We often hear about organizations being data-driven, but I would challenge that healthcare organizations should be people-driven, and by understanding their patient population and integrating data-trained personnel into the healthcare team, you will have better results. With this approach, there might even be a day when no analytical report or dashboard goes unseen or unused 😊
In 2026, I want to focus the theme of the newsletters on quality improvement. How do we design healthcare systems to better serve patients and the community?
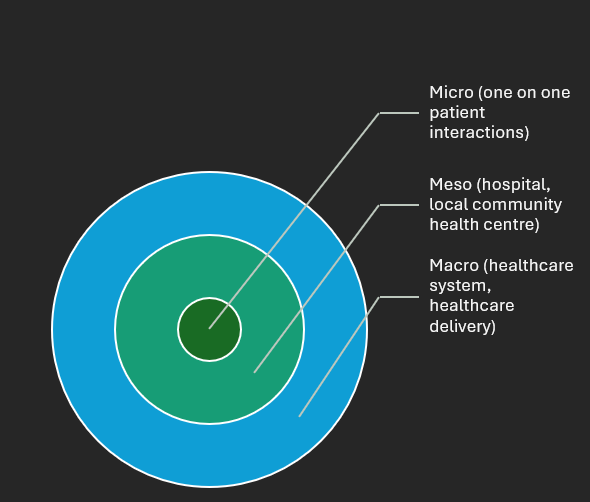
Listening to this podcast episode helped me to understand that when we are thinking about quality improvement and deciding quality metrics, we shouldn’t start at the meso or macro level. If a hospital or local community healthcare system is collecting a set of metrics, another healthcare organization shouldn’t just start collecting the same metrics as they are. The main focus should be to go into the community and understand the metrics that you need to be collecting on a micro level. This bottom-up approach is key.
I’ll leave you with this powerful quote:
“When they train ATAPs (community health workers) and REDES (medical data clerks) in data collection, they tell them, ‘this information is important for you as a healthcare professional, not because it is important to send to the central level, but because you know that you need this information about as much of your population as possible. (Scholar, Department of Public Health, University of Costa Rica).”
0 Comments